





Dina Visca, Simon Tiberi, Emanuele Pontali, Antonio Spanevello, Giovanni Battista Migliori
European Respiratory Journal 2020 56: 2001998; DOI: 10.1183/13993003.01998-2020
COVID-19 affects healthy individuals, patients and healthcare professionals, as well as tuberculosis services. The importance of digital technologies and the impact on quality of life are discussed. https://bit.ly/2U8nA0h
Introduction: the COVID-19 “storm” on individuals, patients and healthcare professionals
The year 2020 will be remembered as the year coronavirus disease 2019 (COVID-19) swept the world and overwhelmed healthcare systems, demonstrating several vulnerabilities and a lack of capacity.
The COVID-19 “storm” has created much damage and will hopefully end (with or without secondary waves, we do not yet know), leaving us in an aftermath with numerous challenges for those involved (table 1).
TABLE 1
The challenges and changes facing healthcare staff and patients during the coronavirus disease 2019 (COVID-19) epidemic
COVID-19 has had a severe impact on a number of parties. For healthy individuals, there has been the worldwide implementation of social distancing measures, lockdown, an unprecedented economic crisis with resultant unemployment, and a feeling of not knowing when it will end. This has generated anxiety and an increase in mental health issues, and in some cases has led to suicide.
With regard to patients, numbers have varied globally, with increased mortality amongst the elderly and patients with pre-existing comorbidities. The socioeconomic consequences of the storm are contributing to increased poverty, deprivation, isolation, malnutrition and related morbidity and mortality.
And for healthcare professionals, the situation has been a nightmare: the request to focus on COVID-19 as a priority; redistribution of healthcare workers into clinical duties; devoting all their energy to preventing, diagnosing and treating this new disease, with limited possibilities to rest and enjoy their family. All this whilst observing an unprecedented pressure on the health system and seeing many colleagues admitted (3.8% in China, 6% in the UK, 10% in Spain) and, unfortunately, dying.
A common occurrence that has been the subject of debate in several medical journals is the rapid reorganisation of health systems to tackle the COVID-19 pandemic by increasing the number of intensive care unit (ICU) beds, and reducing/cancelling out-patient activities and non-urgent clinical activities (e.g. screening and follow-up activities, elective surgery, etc.). Another important shift was to substitute, in whichever way possible, clinical examinations and “in person” meetings with phone consultations and web-based activities.
In many countries, pulmonologists, and infectious disease and public health experts (those also involved in tuberculosis (TB) prevention and care) together with ICU specialists are or have been re-deployed to the frontline to fight COVID-19.
COVID-19 and TB services
A modelling analysis commissioned by the STOP TB Partnership (Geneva, Switzerland) has indicated that the COVID-19 pandemic is deeply affecting the efforts of TB services in prevention, case detection and management. This is particularly evident in resource-limited settings, but can also be seen to varying degrees in resource-rich settings. As a result, an increase in TB incidence and mortality is expected in the future, potentially compromising the results achieved so far and delaying the End TB Strategy timelines.
Discussion about the association between COVID-19 and TB is ongoing. Analysis of two cohorts of co-infected patients has shown that COVID-19 can appear before, simultaneously or after TB (and this includes patients with post-TB treatment sequelae) and that mortality is higher amongst elderly TB patients with pre-existing comorbidities.
Two interesting topics are generating a great deal of scientific debate: the effects of TB on the quality of life (QoL) of TB patients with or without COVID-19 before, during and after anti-TB treatment (with the need for pulmonary rehabilitation); and the potential offered by web-based approaches to TB management.
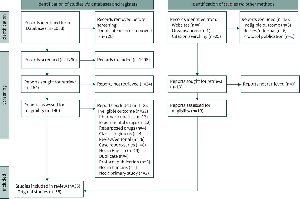
We aim to discuss these two areas by presenting two articles that appear in this issue of the European Respiratory Journal (ERJ), and by making a rapid review of the evidence available on TB, QoL and TB rehabilitation in the literature by searching on Medline, as well as in the grey literature. The keywords “quality of life”, “pulmonary rehabilitation” and “tuberculosis” were used without any time limits.
TB, QoL and pulmonary rehabilitation
51 records were identified, including a review focused on the effectiveness of pulmonary rehabilitation in patients with post-treatment sequelae, five original articles and one case report, reporting both pre- and post-TB rehabilitation information for at least one core examination (i.e. spirometry, walking test, QoL tests). The studies all reported in English, were conducted in four continents (Africa, Asia, Europe and Latin America) with a small sample size (1–64 patients) and 50% of them were on an in-patient basis. The 6-min walking test (6MWT) or equivalent was conducted in all studies, as well as QoL tests. The mean distance covered with the 6MWT was significantly higher after pulmonary rehabilitation, ranging 11–110 m.
Spirometry was conducted in five studies and demonstrated improvement in the core spirometry parameters (forced expiratory volume in 1 s and forced vital capacity) after pulmonary rehabilitation, although age and smoking habits differed in the studies.
Among the main messages of the existing review, we underline: 1) the high proportion of patients with post-TB treatment sequelae with a limited capacity to perform exercise and a poor QoL; 2) the effectiveness of pulmonary rehabilitation in improving walking distance (6MWT), the QoL assessment and core spirometry parameters; and 3) the need for further research.
The importance of QoL in TB has increased over time. According to the World Health Organization (WHO), health is “a state of complete physical, mental, and social wellbeing and not merely the absence of disease or infirmity”.
Therefore, QoL has a precise role in the WHO-recommended vision of “people-centred care”, which is built in to the End TB Strategy.
The traditional vision of national TB programmes focused on improving treatment success rates more than on individual post-treatment wellbeing, largely due to historical funding constraints. In recent years, and before the COVID-19 pandemic, more and more countries (beginning with Brazil, Russia, South Africa and other intermediate-income countries) have shown an interest in rehabilitation for post-treatment sequelae due to increased access to funding and technology.
Among the different QoL tools reported in the literature, there are generic questionnaires such as the 36-item Short-Form Health Survey (SF-36) and its shortened version with 12 questions, or specific tools such as the St Georges's Respiratory Questionnaire that are specifically used to investigate QoL in chronic respiratory diseases (tables 2 and 3).
TABLE 2
Generic tools to evaluate health-related quality of life (HRQoL) in chronic respiratory diseases
Tools to evaluate health-related quality of life (HRQoL) for specific chronic respiratory diseases
QoL, treatment outcomes and the EUROHIS-QOL questionnaire
Amongst the available questionnaires, the EuroQol 5 Dimensions and the SF-36, which are used to calculate quality adjusted life years have been also used in TB. Unfortunately, they cannot capture the economic and social “areas” that are important for TB, given its relationship with poverty and isolation.
The WHO QoL group developed a 100-item questionnaire able to capture different QoL aspects in different cultural environments and with different languages. Shorter versions were also developed for operational research and clinical use, such as the 24-question WHOQOL-BREF and the eight-question EUROHIS-QOL questionnaire. Both tools assess the four QoL core dimensions that are relevant for TB patients: physical health, psychological health, social interactions and satisfaction with living conditions, including economic QoL. The EUROHIS-QOL is a brief questionnaire with the potential of retaining the psychometric properties of WHOQOL-BREF; however, it has only been used to evaluate QoL in a few conditions.
In this issue of the ERJ, Datta et al. report on QoL and treatment outcomes in a case–control, nested cohort of patients. The study was performed in different settings (rural and urban) in Peru and involved: 1545 patients, these were individuals >15 years of age who were initiating anti-TB treatment in community health centres; 3180 “contacts”, these were individuals who reported sharing a patient's household for >6 h per week in the 2 weeks preceding the patient commencing anti-TB treatment; and 277 “controls”, individuals who were randomly selected from within the same communities. The sample size, evaluated post hoc, ensured >90% power at the 95% significance level to detect a 4-point QoL score difference in patients versus controls, and a 1-point difference in contacts versus controls.
The study results indicate that the EUROHIS-QOL eight-item questionnaire is a valid instrument to measure general QoL in TB patients. The vast majority of patients completed it, showing that the questionnaire is reliable and therefore a valid tool to evaluate QoL in these patients. Importantly, patients with TB (and especially multidrug-resistant (MDR)-TB) had lower QoL than community controls as far as TB symptoms and psychosocial QoL dimensions were concerned. TB patients with lower QoL at diagnosis were less likely to complete their TB treatment cycle and survive. The study also allowed for the evaluation of QoL among the patient's household contacts.
This study shows that programmatic QoL evaluation is feasible and can be conducted with simplified tools to improve the outcomes of TB and MDR-TB treatment.
Adherence and e-health
Adherence is a core component of TB treatment, as the traditional dogma of TB control is that rapid and effective treatment is the best preventive measure to reduce infectiousness and break the chain of transmission within the community.
From this perspective, good adherence is key to ensuring a high success rate at the end of treatment, and directly observed therapy (DOT) or its electronic version, video-observed therapy (VOT), are important tools to supporting this.
In this issue of the ERJ, Ravenscroft et al. evaluate the effectiveness of VOT for the first time in low- and middle-income countries. The authors evaluated the effectiveness and patient cost-difference of VOT by comparing VOT with clinic-based DOT in Moldova. The study was designed as a two-arm randomised trial, including 98 cases (VOT group) and 99 controls (DOT group) with observed medication adherence (measured by the number of days per 2-week period that a patient failed to be observed taking medication).
The authors found that VOT significantly decreased non-adherence by 4 days per 2-week period (5.24 days missed per 2-week period for DOT and 1.29 for VOT). From an economic perspective, VOT patients spent approximately €25 and 58 h less on their treatment than DOT patients. As in the majority of DOT studies, no significant improvements were seen amongst VOT patients with regard to treatment success, patient wellbeing or patient employment status.
The main messages of this study are: VOT is feasible in an Eastern European setting, it saves patients' time and money and increases satisfaction. These results are useful and justify larger studies (the sample size was relatively small) that evaluate programmatic feasibility. This is even more relevant in the context of the COVID-19 pandemic, when the prevention of transmission and the need to focus on essential services has reduced the volume of outpatient activities. This, unfortunately, is affecting TB activities in several countries. An additional important result is the increase in the reporting of adverse events. This needs to be seen as a positive “effect” of VOT, which allows otherwise unemerging adverse events to be reported, as recommended by WHO.
Conclusion
A lack of staff, protective equipment, tests and drugs are all well known in the management of TB in diverse settings; this has now unfortunately spread to other programmes and systems. COVID-19 will invariably affect the lung health of many and potentially lead to a greater incidence of TB over the coming years. It is already evident that the pandemic has delayed our ambitious End-TB Strategy timelines, so that greater attention and investments will now be needed to control TB.
The rehabilitation and QoL of TB patients is gaining traction as we understand that patients continue to have sequelae beyond TB treatment completion, and more effort is required to improve QoL and raise life expectancy in this group of patients.
COVID-19 is radically changing the way we manage TB in the immediate future and is forcing us to accelerate the adoption of digital innovations that simplify and facilitate the workload of healthcare workers. COVID-19 has also unmasked and laid bare several vulnerabilities already well known in the TB world; innovation and digital technologies will need to be adopted to help us get back on track.
Acknowledgements
The authors wish to thank Rosella Centis and Lia D'Ambrosio for their technical support in drafting the article and for their useful comments on the manuscript.
Footnotes
-
Conflict of interest: D. Visca has nothing to disclose.
-
Conflict of interest: S. Tiberi has nothing to disclose.
-
Conflict of interest: E. Pontali has nothing to disclose.
-
Conflict of interest: A. Spanevello has nothing to disclose.
-
Conflict of interest: G.B. Migliori has nothing to disclose.
- Received May 26, 2020.
- Accepted May 29, 2020.
- Copyright ©ERS 2020









{kind=link}